1. BONES
(Use articulated skeletons & bone sets) 1.1. Identify the shaft of the femur and the linea aspera


1.1.1. What muscles are attached to the linea aspera?
laterl lip of vastus lateralis
medial lip of vastus medialis
short head of biceps femoris
1.2. What is calcar femorale?

its a dense vertically orientated bone that originates in posteromedial portion of femoral shafts under lesser trochanter; it radiates laterally toward posterior aspect of greater trochanter
The calcar femorale is a spur of thickened bone that lies deep to the lesser trochanter but posterior to the neutral axis of the femoral neck. The calcar is thickest medially where it joins the compression buttress of the neck and gradually thins as it passes laterally. X-ray films taken at right angles to the neutral axis of the femoral neck best portray the calcar femorale, which stands out like a solid bone spur as if viewing along the line of a picket fence. The presence of the calcar femorale affects the configuration of peritrochanteric fractures. It should not be confused with the primary medial compression buttress of the femoral neck -PUBMED
1.2.1. What is its importance?
It reinforces the femoral neck posteroinferiorly and thus protects against trochanteric fracture of osteoperotic femur
1.3. Identify the femoral condyles
1.3.1. What is the medicolegal importance of the centre of ossification of the distal end of the femur?
it emerges just before birth and so is used as medicolegal evidence if an infant is found dead. it will determine wether the infant was viable and near full term.
2. FEMORAL TRIANGLE
2.1. Identify the femoral triangle.
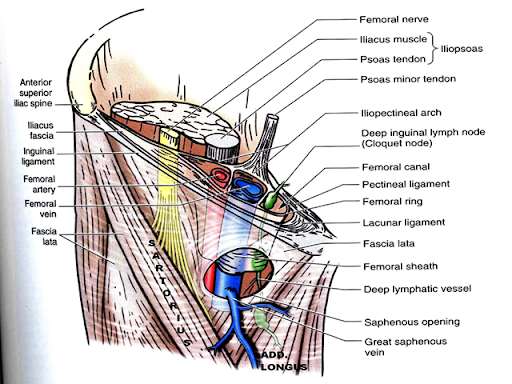
2.1.1. What are its boundaries, roof & floor?
boundaries: sartorius, inguinal ligament, adductor longus
floor: pectineus and illiopsoas
2.1.2. What are its contents?
femoral nerve and vessels
2.2. Identify the femoral sheath
2.2.1. What are its compartments and their contents?
lateral compartment, intermediate compartment, medial compartment
2.2.2. What is the clinical importance of the femoral ring?
femoral hernia
2.3. Identify the superficial (longitudinal & horizontal chain) and deep group of inguinal lymph nodes.

2.3.1. What are their locations & area of drainage?
the superficial lymphatic vessels converge toward and acompany the great sapheneous veins draining into vertical group of inguinal lymph nodes
superficial lymphatic vessels of the lateral foot and posterolateral leg accompany the small sapheneous vein and initially drain into the popliteal lymph nodes- they later drain at the deep inguinal lymph nodes
superficial and deep lymph nodes tranverses the external and common illiac nodes before entering the lateral lumbar (aortic) lymph nodes and the lumbar lymphatic trunk
2.3.2. What is their clinical importance?
enlarged inguinal lymph nodes, lymphadema
3. MUSCLES (Use models, plastinated specimens, articulated skeleton with muscle markings)
3.1. Draw a labelled diagram of a cross-section of the thigh outlining its compartments and contents.

3.1.1. What is the nerve supply to each of these compartments?
anterior- femoral nerve
medial- obturator nerve
posterior- tibial part of sciatic nerve

3.2. Identify Sartorius and its attachments
ASIS & medial proximal tibial shaft via pes anserina
3.2.1. What is its nerve supply?
femoral nerve
3.2.2. What is its function?
flexes and externally rotates hip, flexes knee (tailors position)
3.2.3. What is the space /canal deep to it?
adductor canal
3.2.3.1. What are its contents?
femoral vessels
saphoneus nerve
nerve to vastus medialis
3.2.3.2. What is its clinical importance?
it is usually exposed and ligated in a patient with a popliteal aneurysm as the artery is healthy and will not tear. tying the artery directly above the aneurysm might cause a tear.
3.3. Identify vastus medialis.
3.3.1. Which muscle is it part of?
biceps femoris
3.3.2. What are the other three parts?
rectus femoris
vastus lateralis
vastus intermedius
3.3.3. What is their nerve supply?
femoral nerve
3.3.4. What is their function?
knee extensor, flexes the hip, prevents patella dislocation
3.3.5. Review their attachments.
patella base via quadriceps tendon, then from patella apex to patellar tendon & tibial tuberosity
3.4. Identify adductor brevis.

3.4.1. What splits to surround it?
obturator nerve
3.4.2. Which muscle is superficial to it?
abductor longus
3.4.3. Which muscle is deep to it?
abductor magnus
3.4.4. Which nerve supplies them?
obturator nerve
3.5. What is unusual about adductor magnus?
abductor magnus has an oblique abductor part and a vertical hamstring part. abductor part supplied by obturator nerve wherelse vertical hamstring part is supplied by the tibial nerve
3.5.1. Why should this happen?
lies on border between 2 compartments
3.5.2. Explain why magnus is an atavistic muscle
In other tetrapods, the adductor magnus crosses the knee joint and inserts into the tibia. In humans, the distal part of the tendon detaches and becomes the medial collateral ligament of the knee. Because of this, the medial collateral ligament of the knee in humans may contain a few muscle fibres as an atavistic variation
3.6. What is the adductor hiatus?
gap in the adductor magnus transmitting femoral vessels to/from popliteal fossa
3.6.1. What are the equivalent adductor muscles in the upper limb?
coracobrachialis
3.7. Identify the Hamstring muscles.
Posterior compartment of thigh
Semimembranosus, semitendinosus, biceps femoris long head
3.7.1. What are the characteristic features and common origin of hamstring muscles?
Ischial tuberosity is the common origin. The characteristic feature is that all the muscles flex the leg at knee and extend the thigh at hip joint. (acts on 2 joints)
3.7.2. What is their nerve supply?
tibial division of sciatic nerve
3.7.3. Why do the hamstrings commonly tear?
During sprinting the hamstring muscles work extremely hard to decelerate the tibia (shin bone) as it swings out. It is in this phase just before the foot strikes the ground that the hamstrings, become injured as the muscles are maximally activated and are approaching their maximum length.
3.7.4. How does a slash of the tendons of the posterior thigh muscles (“hamstringing”) at the knee
prevent someone from running?
prevent someone from running?
The slashing of the tendons causes inability to flex the knee and extend the hip, which is a requirement to enable running.
3.7.5. Where do they insert?
semitendinous- surface via pes anserine, semimembranous- medial condoyle of tibia (the back)
3.7.6. What are the extensions of the semimembranosus insertion?
to lateral capsule, oblique popliteal ligament, popliteus fascia, soleal line of tibia
3.7.7. Some people can easily touch their toes with knees kept straight, while others find it difficulty – explain why.
variation in length of hamstrings
3.8. Identify the short head of biceps
3.8.1. Where does the short head of biceps arise?
Lateral lip of linea aspera
3.8.2. Why is it not considered as a hamstring?
The short head of the biceps femoris is not considered a “true hamstring” because it does not attach at the ischial tuberosity and does not produce hip extension. Rather, the short head of the biceps femoris contributes to knee flexion and can also assist with external rotation of the lower leg.
3.8.3. What does this tell you about its development?
the short head was originally an extensor that migrated
the short head was originally an extensor that migrated

4.1. Identify the lateral cutaneous nerve of the thigh
4.1.1. From which division of the lumbar plexus is it derived?
dorsal division of ventral rami of L2 & L3
4.1.2. What other terminal branch, is derived from the dorsal division though it supplies the anterior thigh?
femoral nerve
4.1.2.1. What would be the effects of this terminal branches’ injury?

it would effect the sartorius and illiacus muscle as they are supplied by L2 and L3, since they are in the anterior compartment therefore there will be weak flexion of thigh and loss of sensory at the anterior and medial portion of thigh
4.1.3. What is meralgia paresthetica/ "Jeans disease"?
injury to lateral cutaneous nerve of thigh (LCNT) as it passes deep to inguinal ligament. compression at this area will cause pain, tingling, numbness area of upper anterolateral thigh. this diseaseis usually caused by low cut jeans (mostly females affected)
4.2. Identify the obturator nerve
4.2.1. What is its root value?
L2-L4
4.2.2. What is its relationship to the psoas muscle tendon?
runs along medial border of psoas and along pelvic wall (can be injured in pelvic surgery)
4.2.3. What is its motor and sensory supply?
adductors of thigh (medial compartment) -motor
medial thigh- sensory
4.2.4. Why can hip disease present with pain in the knee?
because of reffered pain as the obturator nerve supplies to both hip and knee
5. VESSELS
5.1. Identify the femoral artery.
5.1.1. Where does it originate?
It is a continuation of external iliac artery distal to the inguinal ligament.
It is a continuation of external iliac artery distal to the inguinal ligament.
5.1.2. What are its major branches?
Deep artery of the thigh (profunda femoris) giving rise to medial circumflex femoral artery and lateral femoral artery
descending genicular, external pudendals, superficial circumflex illiac, superficial epigastric
descending genicular, external pudendals, superficial circumflex illiac, superficial epigastric
5.1.3. At what location does it terminate?
Terminates as it traverses adductor hiatus,where it is named as popliteal artery.
Add a comment